




Arama yapın
Stone disease is an important health problem due to its frequent recurrence and high incidence. It is seen more frequently in some societies due to geographical structural differences, racial differences and genetic structure. Turkish society is also one of the societies where stone disease is frequently seen due to the reasons mentioned above. Urinary system stones are hard formations seen in the kidneys or urinary tract. They form over time due to the crystallization and accumulation of substances that cannot be dissolved and excreted in the urine. If substances such as calcium oxalate or uric acid are present in the urine at higher concentrations than normally expected, a kidney stone forms. These substances can settle in the kidney in the form of crystals and over time they grow to form a kidney stone. Stones can move or be excreted from the body by moving down the urinary tract. However, stones that get stuck in any part of the urinary tract and obstruct the flow of urine generally cause the dreaded, severe typical kidney pain.
Anatomical Abnormalities
B-Environmental Factors
| Calcium oxalate, phosphate or both | %70-80 |
| Struvite (Infection) | %10-15 |
| Uric Acid | %5-10 |
| Cystine | %1 |
| Others (Xanthine, Silicate, Indinavir, Triamterene) | %1 |
Although there are many factors that play a role in stone formation in a person, the exact cause is not fully known.
Potassium citrate works as a urine alkalinizer, preventing the formation of kidney stones before they form.
It is effective in all types of stones except struvite stones.
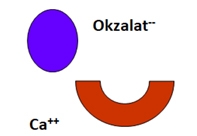
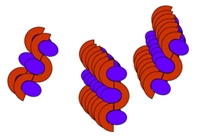
1) Firstly, calcium and oxalate ions are required for the formation of a calcium oxalate (CaOx) stone.
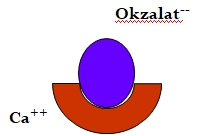
2)To crystallize, two ion pairs need to come together to form CaOx salt
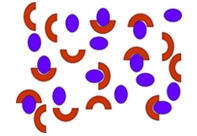
3) Crystallization can only begin when the ion pairs in the environment exceed a certain density.
4) The coming together of ion pairs formed above a certain density (nucleation) is the first step for the formation of a stone.
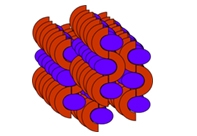
5)However, nucleation alone is not sufficient for stone formation. The formed nuclei also need to come together in an aggregation.
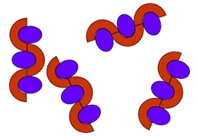
6) Eventually, the stone forms by aggregates piling up on top of each other or accumulating on other aggregates.
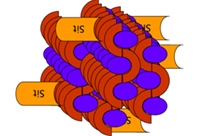
7)However, if citrate is in the environment, it can bind in a way that prevents the formation of the CaOx ion pair. This shows an effect that inhibits nucleation and aggregation formation.
8) The binding of citrate in this way has an inhibitory effect on nucleation and aggregation formation.
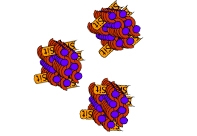
9) Citrate binds to the aggregates that will come together and form a stone, preventing the aggregates from coming together or growing on the aggregate as nucleation.
10) 12. With this inhibitory effect, citrate prevents stone formation.
PATIENTS REDUCE OXALATE INTAKE
Foods rich in oxalate::
Spinach, Tomato, Mustard, Swiss Chard, Strawberry, Chocolate, Sweet Potato, Hazelnut, Peanut
REDUCE SODIUM
Foods rich in sodium:
Table Salt, Packaged Ready-to-Eat Foods, Food Additives, Fast Food, Delicatessen, Salad Dressings, Soy Sauce, Pickle Juice, Chips, Olives
LIMIT ANIMAL PROTEINS
Foods rich in calcium:
Red Meat, White Meat, Offal, Egg, Shellfish, Dairy Products
GET ENOUGH CALCIUM
Cheese, Almonds, Hazelnuts, Peanuts, Soybeans, Green Vegetables, Yogurt
GET ENOUGH FLUID
Drinking At Least 2.0 Lt Water Per Day Is Recommended. It Is Recommended to Stay Away from Tea, Coffee and Alcohol.
REFERENCES
1. Pak, C. (1987). Citrate and Renal Calculi. Mineral and Electrolyte Metabolism 13, 257-266.
2. Pak, C. (1985). Long-Term Treatment of Calcium Nephrolithiasis with Potassium Citrate. The Journal of Urology 134, 11-19.
3. Preminger, G.M., K. Sakhaee, C. Skurla and C.Y.C. Pak. (1985). Prevention of Recurrent Calcium Stone Formation with Potassium Citrate Therapy in Patients with Distal Renal Tubular Acidosis. The Journal of Urology 134, 20-23.
4. Pak, C.Y.C., K. Sakhaee and C. Fuller. (1986). Successful Management of Uric Acid Nephrolithiasis with Potassium Citrate. Kidney International 30, 422-428.
5. Hollander-Rodriguez, J et al. (2006). Hyperkalemia, American Family Physician, Vol. 73/No. 2.
6. Greenberg, A et al. (1998). Hyperkalemia: treatment options. Semen Nephrol. Jan; 18 (1): 46-57.
Adding {{itemName}} to cart
Added {{itemName}} to cart